Dealing With Extreme Dissociation And Immobilization During Conflict
When Trauma Symptoms Show Up In Your Relationship
Hi friends. I am here with an important, nuanced installment of Dear Dr. Marina today. I'll get right to it.
This reader wrote:
I recently read your post What To Say (Instead of Nothing) If You Shut Down During Conflict and had a follow up question about it. As a result of prior relationship abuse, I’ve developed what I think is a functional neurological disorder or component of PTSD where I have episodes of severe freezing/immobility, dissociation, and sometimes seizure-like activity. These episodes happen when I feel triggered (usually by something relational). This happens sometimes with my partner while we’re having difficult discussions. I do my best to warn her when this is coming on, and we’ve talked about ways she might help me and guidelines to help keep our conversations feeling safer, but I know that it feels awful for her that I shut down and have such an extreme reaction while we’re in conflict or having a hard conversation. Do you have any advice on navigating the impacts of “shut down” when it’s more intense than just not being able to talk or process for a few minutes? I do try to make space for her feelings and validate that it’s difficult for her when this happens. At the same time, it can feel hard to do that when these episodes are so scary and awful for me to experience, as was the past abuse that has led to them.
The painful truth is that even after you survive an abusive relationship and enter a new, healthy one, relics of the old dynamic that often linger. The reader describes substantial trauma symptoms that result in an intense physiological shut down, during which they have reduced access to complex cognition and verbal processing.
In today's Love Note, I will provide an overview of why this type of shut down response can "make sense" in the aftermath of trauma and explore options for partners who want to navigate this pattern with mutual care. It's a long, detailed post today, and it's also a heavy topic. Take care of yourself as you read, stop if you need to, and know that your health and safety matters.
Tonic Immobility
I'll try not to get too technical here, but the response we're exploring today is called tonic immobility. Although the word "freeze" makes total sense to use here, that technically refers to a different behavioral and physiological response in what's called the defense cascade. Freezing is a brief, attentive pause to allow an organism to assess danger. In contrast, tonic immobility occurs after that organism has assessed that there is indeed danger and it is not possible to flee or fight back. While there's some quibbling about what exactly to call each response, the basic process looks like the graph below.
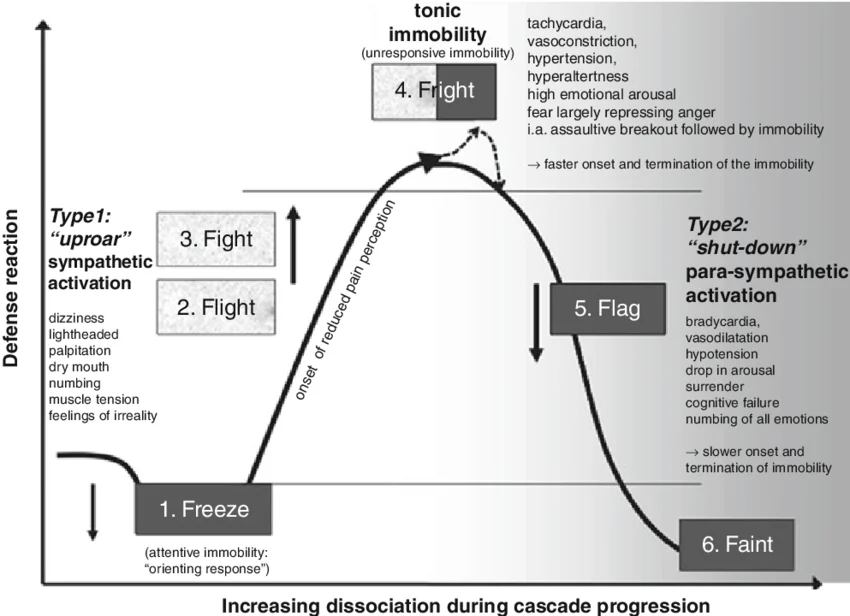
You'll notice in the above graph that there is a continuum between fright and faint in which the body goes from high arousal to low, with the final (potential) mechanism being complete unconsciousness. Notably, tonic immobility is still characterized by high physiological arousal. The person feels frozen, but their heart is racing, their blood pounding. If this state persists, they might proceed to a lower arousal state in which the body is literally shutting down.
As a person progresses along this defense cascade, the presence of dissociation increases. Dissociation is a break down in how you typically perceive and make meaning of your own consciousness and environment. You can dissociate very mildly (seeming slightly spacey or out of it) or dissociate very severely (resulting in complete amnesia or a visceral flashback to a different time in your life).
One more thing to know: the type of defense utilized during a trauma itself very often shows up after the trauma. For example, if you experienced a trauma in which you were able to flee, you may tend to do so when you are activated. If you experienced a trauma in which fighting and fleeing were both impossible, you may tend to go quickly to a dissociative, immobile state.
Tonic immobility and extreme dissociation tend to happen after severe and/or prolonged trauma. On a very basic level, this makes a lot of sense from the perspective of learned helplessness. When attempts to keep yourself safe are repeatedly unavailable, the most "adaptive" option remaining may be to shift the one thing left that you can control: your own consciousness. It's also a way to become uninteresting to a predator in hopes that they eventually leave you alone.
I'll get back to the reader question shortly, but this overview matters because how we understand what is happening will directly inform the options available. How can you be mindful of your partner's needs when your own capacity to communicate goes away completely sometimes? How can a (loving, mutually invested) couple work through this together?
I'm not going to focus on the potential healing steps that a person with these types of symptoms could take, because that's a much bigger topic and should be personalized in the context of individual therapy. But I do want to say that it is possible to move the needle on dissociation and the immobilization response, with time and focused trauma therapy.
In the meantime, however, how can partners stay connected in the face of this sort of extremely physical trauma response?
Patience, Trust, and Safety
This may seem obvious, but all the ideas below will only apply in the context of a safe relationship with a partner who is invested in your health and safety. If the immobilization response is still showing up because this relationship is also unsafe, it doesn't make sense to focus on preventing the response, which the body is still seeing as adaptive.
Assuming you have a safe, loving connection, there are some things that may help, but they will take time. This is work best done with a partner who is willing to be patient and build trust together. Although not impossible, it is very difficult to do this work when the other person's own trauma history and symptoms are activated by the tonic immobility. For example, if your partner's response to their personal trauma means that the absolute most painful, frightening thing for them is when you are completely silent, and they feel a strong need to pursue you to speak and engage...this work will be extra challenging.
Improve Your Baseline
Reactions like tonic immobility can be idiosyncratic such that there may not always be a clear external trigger. Or there may be a visible trigger, but it's something unavoidable that you can't simply prevent. And more broadly, while healing from trauma, it's generally not advisable to use avoidance as a coping strategy (i.e., telling a partner, "it's too upsetting when you disagree with me, please don't" is not a healthy option for anyone involved).
That said, without avoiding normal, natural aspects of being in a relationship, you can tend to the basics to create a calm, regulated baseline.
That might mean focusing a lot on things like:
- Pace of words during conflict—both partners make an effort to speak at a relatively slow cadence
- Pausing after concepts and before jumping in—say one thing at a time, then stop and allow space
- Reflective listening—repeating back what you heard the other person say (potentially after every single idea is expressed)
- Separating thoughts and feelings from problem solving and decision making—not adding pressure to come up with a solution when what's really happening is emotional expression
- Using writing long-form letters as a way to express complex concepts to each other without urgency and increased intensity (do this asynchronously, not via text)
No one ever regrets learning to communicate through conflict with great care and respect, so there's really no downside to focusing, proactively, on creating a very stable, regulated conflict baseline.
Create a Standard Operating Procedure Together
Like we discussed above, triggers are not always predictable or even visible, so they will likely still happen. So, then what?
The reader alludes to having made a plan with their partner, and that's what I would recommend. In fact, I would suggest getting extremely clear about the plan and putting it in writing where it is easily accessible to both people and can be used in the moment. You could even laminate it!
Think about this like a standard operating procedure. Keep it very concrete and action-oriented.
Things to include:
- When you notice early warning signs of becoming dissociative or immobilized, how is that information communicated? Consider a hand signal or single word.
- What happens next, after the distress signal is made? Does the conversation stop fully? Does partner walk away and give space? Is touch or speech okay?
- How do you reconnect if there has been space? How much time is typically needed? Which partner reaches out?
- When do you revisit the hard topic (and how)?
Keep it simple and literal. Imagine yourselves picking up your SOP paper during a crisis moment and trying to figure out what to do next...support your future self by giving specific, targeted guidance.
Express Care After The Fact
Two things are true here. One, it is deeply unpleasant and terrifying to experience an episode of tonic immobility. It often feels like "going back" to the original trauma. And two, it is frightening and frustrating to try to express yourself to your partner and then suddenly find they are completely unavailable (and may need care themself).
You'll both lose again and again if you can't hold space for this duality. In the moment, the focus will appropriately shift to meeting the needs of the person experiencing an acute symptom. And also, the other person is still human with thoughts and feelings.
As part of your SOP (above), make sure to include a way for your partner to get heard and receive care if they need it. Very often, partners are more than willing to defer their own emotional expression when their person is hurting. But what they aren't willing to do, and what will start to wear, is completely silence their own emotions long term. Find avenues, after the reaction has passed, to listen, express care, and engage directly in hard topics. Use the supports you need (therapy, writing back and forth, keeping conversations short and calm)—but also keep letting them know that you are willing to hold space for their experience.
I hope this love note was informative. If any of it resonated, I strongly suggest exploring further with a care provider who knows you and your context. These are heavy topics—take good care of yourself today.
Love Notes for Real Life is reader-supported and affiliate-free.